










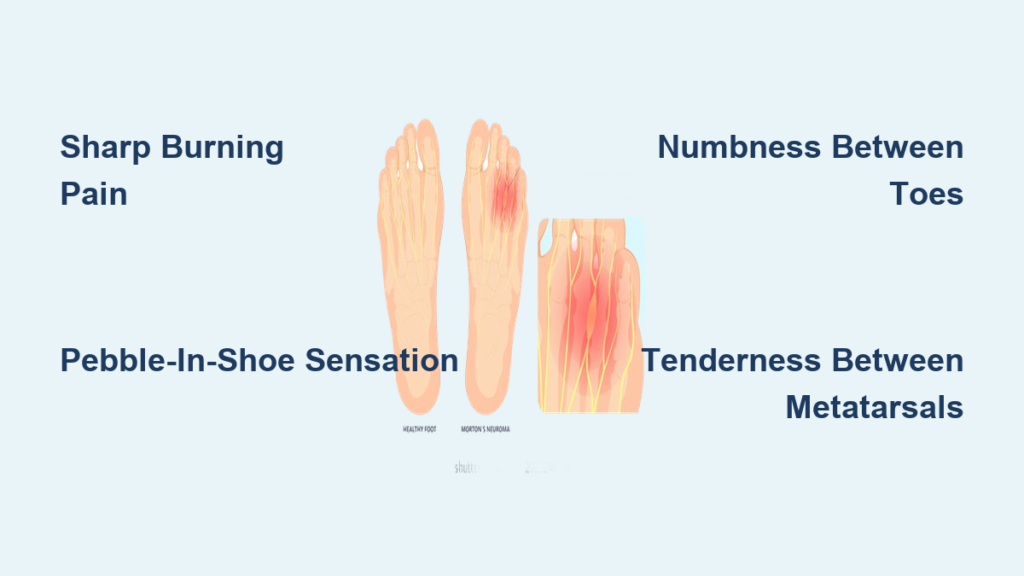
If you’re experiencing sharp, burning pain in the ball of your foot that feels like you’re walking on a pebble—even when barefoot—you may be dealing with a Morton’s neuroma, a common but often misunderstood condition affecting the nerve between the third and fourth toes. This isn’t a true tumor, but rather a thickening of the tissue around the plantar digital nerve due to chronic compression or irritation. Left untreated, it can progress from occasional discomfort to persistent, debilitating pain that alters how you walk and impacts daily life.
Morton’s neuroma typically develops in adults between 30 and 60, especially women who wear high heels or narrow shoes. Athletes, dancers, and individuals with foot deformities like bunions or high arches are also at higher risk. The good news? Early recognition of symptoms can prevent long-term nerve damage and avoid the need for surgery. In this guide, we’ll break down the key signs of a neuroma between the third and fourth toes, how to distinguish it from other foot conditions, and what steps to take next.
Sharp or Burning Pain Under the Ball of the Foot
One of the earliest and most telling signs of a neuroma is sharp, burning pain beneath the metatarsal heads, just behind the third and fourth toes. This pain often feels like:
– A stabbing or electric shock with each step
– A throbbing sensation that radiates forward into the toes
– Increased intensity during weight-bearing activities like walking, standing, or running
The discomfort usually starts intermittently—after long periods on your feet or while wearing tight footwear—but over time, it can become constant. Many patients report that the pain “shoots” into the toes, particularly the third and fourth, confirming nerve involvement rather than general foot soreness.
Pro tip: If the pain flares when you stand on the balls of your feet or pivot quickly (common in tennis or dance), it’s a strong indicator of nerve compression in the third interspace.
When Pain Becomes Constant
In early stages, rest and removing your shoes may provide relief. But as the nerve continues to thicken, episodes become longer, more frequent, and harder to ignore. Eventually, pain may occur even at rest or during non-weight-bearing activities, signaling advanced nerve irritation that requires prompt intervention.
Radiating Pain Into the Third and Fourth Toes
Unlike general forefoot pain, Morton’s neuroma doesn’t stay localized. The discomfort spreads from the ball of the foot into the adjacent sides of the third and fourth toes. This radiation is a key differentiator from conditions like metatarsalgia, which causes diffuse soreness without nerve-like symptoms.
The sensation is often described as deep and internal—more like a nerve firing than surface-level pain. It tends to worsen during activities that involve pushing off the forefoot, such as walking uphill, climbing stairs, or running.
The “Pebble-in-Shoe” Sensation: A Hallmark Symptom
Perhaps the most distinctive sign of a neuroma is the feeling of a marble, stone, or crumpled sock under the foot, even when no object is present. This phantom sensation occurs because the compressed nerve sends abnormal signals to the brain, which interprets them as pressure or a foreign body.
Patients frequently stop mid-walk to check their shoes, only to find nothing there. This symptom is rare in other foot conditions and strongly points to nerve-based pathology like Morton’s neuroma.
Numbness and Tingling Between the Toes
As nerve compression progresses, many people develop paresthesia—a pins-and-needles, buzzing, or crawling sensation between the third and fourth toes. Some report:
– Numbness or loss of feeling on the sides of the toes
– Intermittent tingling that comes and goes
– A “dead” or “asleep” feeling despite no visible injury
These neurological changes confirm that the problem is not muscular or skeletal, but rooted in nerve dysfunction. Unlike temporary numbness from tight socks, this persists and often correlates with activity or footwear.
Risk of Permanent Nerve Damage
If left untreated, chronic pressure can lead to permanent sensory loss. Even after treatment—especially surgical removal—the affected toes may remain numb. Early care significantly improves the chances of full recovery without lasting deficits.
Swelling and Forefoot Fullness
Though not always visible, inflammation around the nerve can cause subtle swelling between the metatarsal heads. You might notice:
– A tight or full feeling in the ball of the foot
– Mild puffiness that worsens by evening
– Tenderness when pressing between the third and fourth toes
This localized swelling contributes to the “crowded” sensation and can make shoe fit uncomfortable, creating a cycle of more pressure and worsening symptoms.
Toe Cramping and Muscle Spasms
Some patients experience involuntary cramping in the toes, especially after prolonged standing or walking. While not directly caused by the neuroma, these spasms result from gait compensation—altering your step to avoid pain—which strains small foot muscles. Over time, this can lead to secondary issues like calf tightness or arch fatigue.
Pain Triggers: What Makes It Worse?
Tight, Narrow, or High-Heeled Shoes
Footwear is the number one trigger for neuroma pain. Narrow toe boxes and heels over 2 inches dramatically increase pressure on the forefoot:
– High heels shift body weight forward, compressing the metatarsal heads
– Pointed shoes squeeze the bones together, pinching the nerve
– Tight athletic footwear (e.g., cycling shoes, ski boots) can initiate or worsen symptoms
Switching to wide, flat shoes often brings noticeable relief within hours.
High-Impact Activities
Sports involving running, jumping, or sudden direction changes—like tennis, basketball, or aerobics—exacerbate the condition. The repetitive impact inflames the nerve further. Dancers, especially those in rigid or tight footwear, are also highly susceptible.
Quick test: Walk barefoot on a soft surface. If pain decreases significantly, it suggests mechanical compression is the culprit.
How Doctors Diagnose a Neuroma

Positive Mulder’s Sign
During an exam, your doctor may perform the Mulder’s squeeze test:
1. Compress the forefoot from side to side
2. Press upward on the space between the third and fourth metatarsals
A distinct “click” or palpable snap, accompanied by radiating pain, is considered positive for Morton’s neuroma. This occurs when the enlarged nerve gets trapped and displaced under the ligament.
Tenderness on Palpation
Direct pressure on the bottom of the third interspace usually reproduces the pain. The spot is often pinpoint tender, and patients may flinch or pull the foot away when touched.
Imaging: Ultrasound vs. MRI
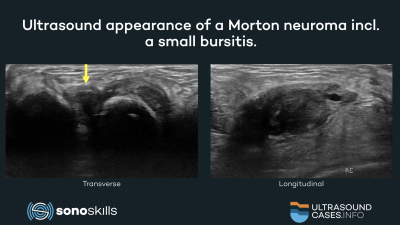
Ultrasound: Fast and Accurate
Ultrasound is highly effective for confirming a neuroma. It can detect:
– Nerve thickening (typically >4 mm diameter)
– Hypoechoic mass in the intermetatarsal space
– Dynamic changes during compression
It’s preferred over MRI in many cases due to lower cost, no radiation, and real-time imaging.
MRI for Unclear Cases
MRI provides detailed soft tissue views and shows:
– T2 hyperintense signal in the affected nerve
– Surrounding inflammation or fibrosis
It’s used when diagnosis is uncertain or to rule out mimics like plantar plate tears or stress fractures. However, imaging isn’t foolproof—some neuromas don’t show up clearly, so clinical judgment remains key.
Conditions That Mimic a Neuroma

Metatarsalgia vs. Neuroma
Metatarsalgia causes generalized forefoot pain but lacks radiating nerve symptoms or the “pebble” sensation. It’s more diffuse and often linked to poor cushioning or overuse.
Stress Fractures
A stress fracture in the third or fourth metatarsal causes localized pain but is usually worse at night and shows X-ray changes over time. Neuroma pain improves with rest and doesn’t appear on X-rays.
Plantar Plate Tears
Tears in the ligament under the toe joint can mimic neuroma pain but often cause visible toe drift or instability, and MRI shows structural damage.
Peripheral Neuropathy
Diabetic or systemic neuropathy causes bilateral, symmetrical numbness starting in the toes. Morton’s neuroma is typically unilateral and localized.
Red flag: Always rule out systemic causes if symptoms are in both feet or accompanied by other neurological issues.
Risk Factors You Can Control
High Heels and Narrow Shoes
Wearing high-heeled or pointed footwear is the top modifiable risk factor. The combination of heel elevation and toe squeezing creates the perfect environment for nerve irritation.
Solution: Switch to shoes with:
– Heel height under 2 inches
– Wide toe box
– Soft, cushioned soles
Even stretching existing shoes can help reduce pressure.
Excess Body Weight
Extra weight increases load on the forefoot with every step. Losing weight—even 10–15 pounds—can significantly reduce symptoms and prevent progression.
Repetitive Forefoot Loading
Runners, dancers, and athletes should incorporate low-impact cross-training (swimming, cycling) and ensure proper footwear with metatarsal support.
When to See a Specialist
Don’t wait for pain to “go away.” See a podiatrist or foot specialist if:
– Pain lasts more than 2 weeks
– You feel numbness or tingling
– Over-the-counter remedies don’t help
– You’ve changed shoes but still have discomfort
Early treatment can avoid injections or surgery.
Final Note: A neuroma between the third and fourth toes won’t heal on its own. But with early recognition and conservative care—like changing footwear, using orthotics, or getting targeted injections—most people avoid surgery and return to pain-free activity. Listen to your feet: unusual sensations are warnings, not just annoyances. Address them early, and you can prevent long-term complications.



